DRX9000® European Musculoskeletal Research 2008
Figure 1

Figures 2

1. Adjunct Assistant Professor, Johns Hopkins University School of Medicine;
2. Director of Clinical Research, NEMA Research Inc.;
3. Assistant Professor,Department of Radiology, Johns Hopkins University School of Medicine;
4. Director of Clinical Research, Axiom Worldwide, LLC; 5. Big Sky Spinal Care Center
Non-surgical Spinal Decompression (DRX9000™) for the Treatment of Chronic Low-back Pain – A Case Report
A report by
1 Joseph Pergolizzi, 2 Charlotte Richmond, 3 Martin Auster, 4 Frank Florio, 5
Jonathan Wilhelm
- Adjunct Assistant Professor, Johns Hopkins University School of Medicine;
- Director of Clinical Research, NEMA Research Inc.;
- Assistant Professor, Department of Radiology, Johns Hopkins University School of Medicine;
- Director of Clinical Research, Axiom Worldwide, LLC; 5. Big Sky Spinal Care Center
Back pain affects millions of workers worldwide. The prevalence of back pain is associated with the number of hours spent on repeated activities at work1 and in high-risk occupations.2 In 1938, it was believed that there was no one condition that produced more disability and economic loss than low-back pain (LBP).3 This statement is just as true today as it was 70 years ago.4–6
Currently, there are abundant options for treatment, with new, often innovative, treatments emerging. However, there is little agreement on which treatment is appropriate or preferable: surgical, non-surgical or pharmacological. Results from back surgery are unpredictable and are associated with surgical risks. Conservative treatment for at least two months, and often much longer, before a surgical option is considered has been recommended in the current evidence-based guidelines.7,8
The American Pain Society’s guidelines on LBP have dismissed some interventions such as invasive diagnostic testing, various spinal injections and fusion surgery for non-radicular pain.9 Results from a pilot study using non-surgical spinal decompression, specifically the DRX9000™ (Axiom Worldwide, Tampa, Florida),10 are promising and offer another option for treatment of chronic LBP. Therefore, a case of chronic LBP successfully treated with non-surgical spinal decompression via the DRX9000® is reported here.
Figure 1
Figures 2
1. Adjunct Assistant Professor, Johns Hopkins University School of Medicine;
2. Director of Clinical Research, NEMA Research Inc.;
3. Assistant Professor,Department of Radiology, Johns Hopkins University School of Medicine;
4. Director of Clinical Research, Axiom Worldwide, LLC; 5. Big Sky Spinal Care Center
Presentation of Case
A 35-year-old female presented at an outpatient clinic in July 2006 complaining of LBP. The back pain was associated with numbness and recurrent right leg pain. The treating physician noted that the patient’s condition had been chronic since December 2004. These symptoms affected her ability to lift clients – a required part of her occupational duties – and were aggravated by sitting and prolonged standing. The patient weighed 291lb and was 5’ 8” tall. Her history was significant, with two motor vehicle accidents (in 1994 and 2002). Magnetic resonance imaging (MRI) of the lumbar spine performed on 19 July 2006 revealed a mild to moderate disc protrusion at L5/S1, eccentric to the right, impinging on the right S1 nerve root (see Figure 1). Mild degenerative changes with minimal bulging were also noted at L2/L3 and L3/L4. Upon initial examination, the patient presented limited lumbar range of motion (ROM), with pain in all planes, positive nerve root tension tests and decreased sensory and motor function of the right lower extremity.
The patient underwent 20 treatments on the DRX9000® over an approximately 5.5-week period. Initial parameters began at a maximum decompressive force of 90lb with a minimum force of 45lb. Final treatment parameters were a maximum of 110lb and a minimum of 55lb. The decompressive force was raised in increments of 10lb at the discretion of the healthcare provider. The angle of treatment force (which allows the physician to make adjustments to treat the affected lumbar region) ranged from 10 to 20º. Adjunctive treatment included electric stimulation, ice and therapeutic exercise.
At initial treatment, the patient reported pain at 7 on a 0–10 scale; at the end of the treatment protocol she reported pain at 1. A reduction in the duration of pain was noted as well: pain initially occurred 75% of the time, but decreased to 10% of the time at completion of treatment. At final evaluation, the examiner noted an improvement in lumbar ROM tests: flexion increased from 42 to 58º, extension increased from 12 to 26º, left lateral flexion increased from 14 to 25º and right lateral flexion increased from 12 to 24º. Orthopaedic and neurological findings were noted as normal. Limited follow-up MRI of the lumbar spine performed on 22 September 2006 revealed a decrease in the excursion of the disc at L5/S1 on T2-weighted sagittal images (see Figure 2).
Discussion
The DRX9000® True Non-surgical Spinal Decompression System™ applies spinal distraction forces by using a sensitive computerised feedback mechanism to provide relief of LBP and symptoms associated with herniated discs, bulging or protruding intervertebral discs, degenerative disc disease, posterior facet syndrome and sciatica.11 In a systematic review of the peer-reviewed literature,12 Macario and Pergolizzi conclude that there are too little data to determine whether spinal decompression provides greater benefit than other non-surgical treatments. However, the results of two new studies suggest that the DRX9000® is safe and efficacious in patients with discogenic LBP.10,13
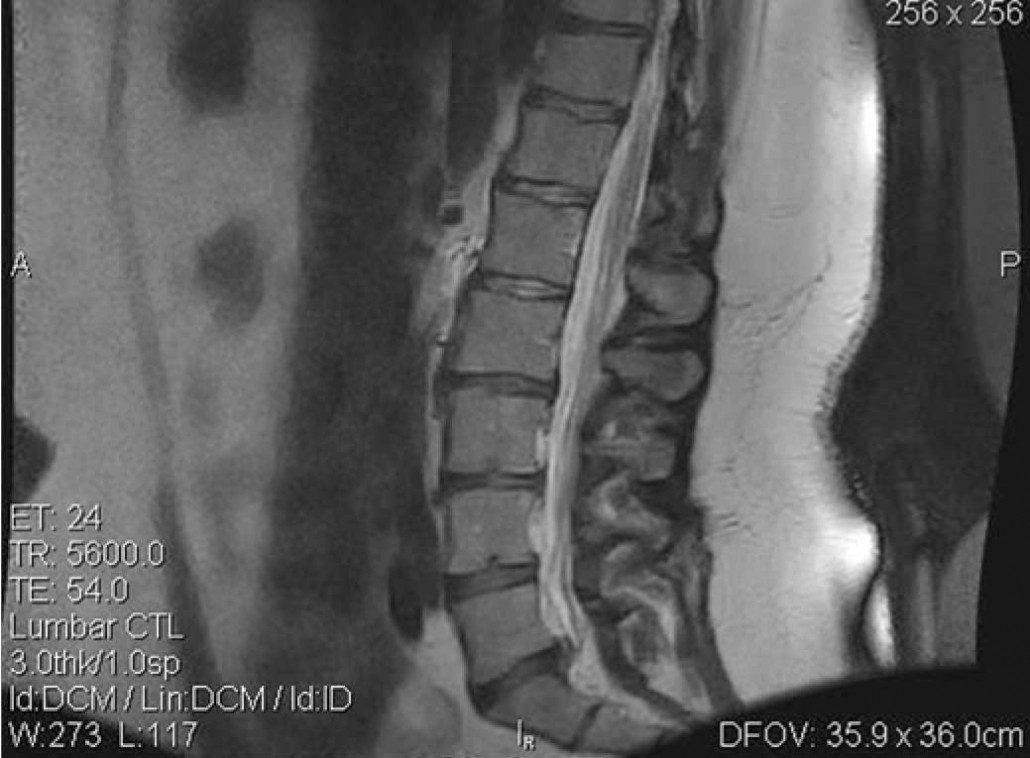
Figure 2: Pre-treatment Magnetic Resonance Image

In the first study, a retrospective study was conducted to evaluate the efficacy of non-surgical spinal decompression using the DRX9000®.13 Ninety-four charts were reviewed from September 2005 to March 2006 at four outpatient clinics (three free-standing and one hospital-based). The mean verbal rating score (VRS) decreased from 6.05 (1–10 scale) at the start of treatment to 0.89 at treatment completion. Similar results were reported in the second study, a prospective, multicentre, non-randomised phase II pilot study to evaluate the safety and effectiveness of the DRX9000® for the treatment of chronic LBP. Eighteen evaluable patients, followed between January 2007 and April 2007, received a 20-treatment protocol with the DRX9000® over a six-week period. Assessments of pain, analgesic use, functionality, satisfaction, activities of daily living and safety were collected through examinations, questionnaires and patient diaries. The mean VRS at the start of treatment was 6.4; it decreased by more than 50% at two weeks (10 treatments) and averaged 0.8 at the end of treatment. Sixteen of the 18 patients reported better function and patients rated the DRX9000® with an average score of 8.1 on a 0–10 satisfaction scale. No adverse events were noted and no subjects required more invasive therapy.
Recently, three case reports addressing the effectiveness of the DRX9000® have been published.14–16 In the first case report,14 a 33-year-old male with an initial VRS of 6 (0–10 scale) received 20 DRX9000® treatments over a sixweek period and reported a decrease in the VRS to 0 at the time of the last treatment. Pre- and post-DRX9000® MRIs were compared, demonstrating an increase in the intradiscal signal on T2-weighted images at L2/3, L3/4, L4/5 and L5/S1, which suggests a positive hydrating effect on the intervertebral disc. The second case report followed a 69-year-old male with chronic LBP radiating to both legs.15 His VRS decreased from 10 to 1 (0–10 scale) with 22 treatment sessions over a seven-week treatment period. Comparison of pre- and post-treatment MRIs demonstrated increased disc height and decreased herniation size at multiple lumbar levels. Comparable results were reported in the third case report, in which a 31-year-old male with a onemonth history of LBP (history of previous episodes of back pain) with radiation into the left buttock received 27 DRX9000® treatments over a seven-week period. VRS decreased from 8.5 to 3 (0–10 scale), with a dramatic decrease in the size of the disc lesion and the compression placed on the left S1 nerve root on post-DRX9000® MRI of the lumbar spine.
The results of these previous case reports, in addition to the results of the current study, are consistent with the results of data retrospectively collected from lumbar spine computed tomography (CT) scans taken prior to and after DRX9000® treatments.17 Sixteen patients with chronic musculoskeletal, mechanical or discogenic LBP received a six-week course of DRX9000®, resulting in a decrease in palpation pain scores of 5.7 to 0.8 (0–10 scale) and ROM pain scores from 5.6 to 0.7. Additionally, the average lumbar disc height was increased by 1.6mm. Furthermore, an increase of 1mm in disc height was associated with a decrease of 3.4 (0–10 scale) for both palpation and ROM pain.
Figure 1: Pre-treatment Magnetic Resonance Image
Figure 2: Pre-treatment Magnetic Resonance Image
In the first study, a retrospective study was conducted to evaluate the efficacy of non-surgical spinal decompression using the DRX9000®.13 Ninety-four charts were reviewed from September 2005 to March 2006 at four outpatient clinics (three free-standing and one hospital-based). The mean verbal rating score (VRS) decreased from 6.05 (1–10 scale) at the start of treatment to 0.89 at treatment completion. Similar results were reported in the second study, a prospective, multicentre, non-randomised phase II pilot study to evaluate the safety and effectiveness of the DRX9000® for the treatment of chronic LBP. Eighteen evaluable patients, followed between January 2007 and April 2007, received a 20-treatment protocol with the DRX9000® over a six-week period. Assessments of pain, analgesic use, functionality, satisfaction, activities of daily living and safety were collected through examinations, questionnaires and patient diaries. The mean VRS at the start of treatment was 6.4; it decreased by more than 50% at two weeks (10 treatments) and averaged 0.8 at the end of treatment. Sixteen of the 18 patients reported better function and patients rated the DRX9000® with an average score of 8.1 on a 0–10 satisfaction scale. No adverse events were noted and no subjects required more invasive therapy.
Recently, three case reports addressing the effectiveness of the DRX9000® have been published.14–16 In the first case report,14 a 33-year-old male with an initial VRS of 6 (0–10 scale) received 20 DRX9000® treatments over a sixweek period and reported a decrease in the VRS to 0 at the time of the last treatment. Pre- and post-DRX9000® MRIs were compared, demonstrating an increase in the intradiscal signal on T2-weighted images at L2/3, L3/4, L4/5 and L5/S1, which suggests a positive hydrating effect on the intervertebral disc. The second case report followed a 69-year-old male with chronic LBP radiating to both legs.15 His VRS decreased from 10 to 1 (0–10 scale) with 22 treatment sessions over a seven-week treatment period. Comparison of pre- and post-treatment MRIs demonstrated increased disc height and decreased herniation size at multiple lumbar levels. Comparable results were reported in the third case report, in which a 31-year-old male with a onemonth history of LBP (history of previous episodes of back pain) with radiation into the left buttock received 27 DRX9000® treatments over a seven-week period. VRS decreased from 8.5 to 3 (0–10 scale), with a dramatic decrease in the size of the disc lesion and the compression placed on the left S1 nerve root on post-DRX9000® MRI of the lumbar spine.
The results of these previous case reports, in addition to the results of the current study, are consistent with the results of data retrospectively collected from lumbar spine computed tomography (CT) scans taken prior to and after DRX9000® treatments.17 Sixteen patients with chronic musculoskeletal, mechanical or discogenic LBP received a six-week course of DRX9000®, resulting in a decrease in palpation pain scores of 5.7 to 0.8 (0–10 scale) and ROM pain scores from 5.6 to 0.7. Additionally, the average lumbar disc height was increased by 1.6mm. Furthermore, an increase of 1mm in disc height was associated with a decrease of 3.4 (0–10 scale) for both palpation and ROM pain.
Conclusion
This case report continues to demonstrate the positive effects of the DRX9000® on disc morphology. This 35-year-old woman experienced pain relief and a decrease in herniation size following 20 treatments over an approximately 5.5-week period. These findings are consistent with previous case reports14–16 of patients successfully treated with the DRX9000® and with a retrospective CT review study.17 Results of these case reports and retrospective study suggest that additional prospective clinical trials are needed.
References
- Guo HR, Working hours spent on repeated activities and prevalence of back pain, Occup Environ Med, 2002;59(10): 680–88.
- Guo HR, Tanaka S, Cameron LL, et al., Back pain among workers in the United States: national estimates and workers at high risk, Am J Ind Med, 1995;28(5):591–602.
- Gilcreest EL, Lumbosacral and sacro-iliac strain causing low back pain: a review of one hundred fifty cases, Ann Surg, 1938;107(6):988–95.
- Deyo RA, Mirza SK, Martin BI, Back pain prevalence and visit rates: estimate from US national surveys, 2002, Spine, 2006;31: 2724–7.
- Krishnaney AA, Park J, Benzel EC, Surgical management of neck and low back pain, Neurol Clin, 2007;25:507–22.
- Jarvik JG, Deyo RA, Diagnostic evaluation of low back pain with emphasis on imaging, Ann Intern Med, 2002;137:586–97.
- Chou R, Qaseem A, Snow V, et al., Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society, Ann Intern Med, 2007;147:478–91.
- McCamey K, Evans P, Low back pain, Prim Care, 2007;3:71–82.
- Marcus A, APS guidelines on low back pain dismiss some interventions, Pain Med RSS, 2008;34:07.
- Leslie J, Richmond C, Macario A, et al., Pilot: Effectiveness and safety of non-surgical spinal decompression, Paper presented at the 18th Annual Meeting of the American Academy of Pain Management, Las Vegas, NV, 27–30 September 2007.
- Gan TJ, Leslie J, Pergolizzi J, Non-surgical Spinal Decompression to treat chronic low back pain, Special Report supplement featured in Anesthesiology News, December 2007.
- Macario A, Pergolizzi J, Systematic literature review of spinal decompression via motorized traction for chronic discogenic low back pain, Pain Pract, 2006;6:171–8.
- Macario A, Richmond C, Auster M, Pergolizzi JV, Treatment of 94 outpatients with chronic discogenic low back pain with the DRX9000®: a retrospective char review, Pain Pract, 2008;8:
11–17. - Richmond C, Florio F, Wilhelm JM, et al., MagneticResonance Imaging Findings after Treatment with a Non-surgical Spinal Decompression System (DRX9000™)—Case Report, USMusculoskeletal Review, 2007;50–52.
- Pergolizzi J, Florio F, Martin W, et al., Management of low-back pain with a non-surgical spinal decompression system (DRX9000™) – case report, European Musculoskeleta review, 2008;59–60.
- Pergolizzi J, Yocum T, Florio F, et al., Management of discogenic low-back pain with a non-surgical decompression system (DRX9000™)—Case Report, US Musculoskeletal Review, 2008;14–15.
- Apfel C, Cakmakkaya S, Martin W, et al., Decreased lower back pain after non-invasive spinal decompression may be due to restored disc height, Abstract presented at the American Conference on Pain Medicine 3rd A
