The Effect of Rehabilitation Exercises Using DRX9000 Spinal Decompression Device on the Rehabilitation of Lower Back Pain in Athletes Who Use Wheelchairs
Pubmedia Journal Pendidikan Olahraga, Vol: 3, No 1, 2025, Page: 1-11 | Published: 30 September 2025
Table 1
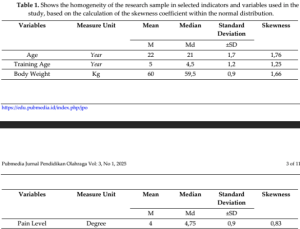
Table 2
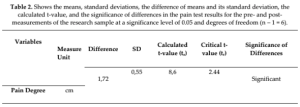
Table 3
Rosemont, IL; 2018.
The Effect of Rehabilitation Exercises Using DRX9000 Spinal Decompression Device on the Rehabilitation of Lower Back Pain in Athletes Who Use Wheelchairs
Please see the full study here.
Abstract
Sports injuries are considered a significant issue for athletes in general and for individuals with disabilities in particular, as they represent a major factor affecting the physical performance of disabled individuals who engage in sports and physical activities. People with disabilities already experience limitations and reduced mobility due to their impairments, which increases their risk of injury during physical activity, whether from improper movements or actions that exceed their natural physical capacity. One common injury among wheelchair users in various sports is lower back pain, characterized by the onset of pain and limited mobility in the lumbar region. This condition can impede athletic performance, leading to temporary cessation of sports activities until the pain subsides. Recurrent episodes may result in complications or more severe injuries. Even minor lower back pain, if not addressed with appropriate medical and therapeutic measures, can develop into a serious condition. Through a review of existing literature, the researcher observed that current rehabilitation and treatment programs for lower back injuries may not adequately meet the specific needs of individuals with disabilities. Therefore, the researcher designed a set of exercises tailored to the physical capabilities of wheelchair users, incorporating the programmed spinal traction device (DRX9000) and additional assistive tools, under the supervision of a specialized orthopedic physician and physiotherapy experts.
INTRODUCTION
This study includes a set of rehabilitative exercises designed to restore the lumbar spine (lumbar vertebrae) and the associated muscles through a series of physical exercises combined with the electronic spinal traction device (DRX9000). This device is unique in that it applies spinal traction based on a graphical curve that specifies the degree of traction and the targeted vertebrae. The DRX9000 is a modern device that helps restore the correct anatomical alignment of the vertebrae and alleviates pain, allowing the exercises to be performed without discomfort. It also promotes proper strengthening of the muscles supporting the lumbar region and ensures that movements are performed within their normal functional range (Zhang, 2021).
The rehabilitation program lasted for 50 days and involved a group of wheelchair-bound athletes participating in various sports for individuals with disabilities who suffer from lower back pain. Their conditions were diagnosed by a specialist as mild lumbar disc herniation, requiring rehabilitative exercises to prevent the worsening of the condition and the progression of the injury.
The problem addressed in this study is that most rehabilitation programs are not specifically designed for individuals with disabilities, and modern devices are rarely utilized in treatment. This often prolongs therapy and can cause boredom among patients, especially since these individuals have special needs and require rehabilitation programs tailored to their physical and psychological conditions (Schenck, 2022).
The aim of this study is to evaluate the effectiveness of the designed rehabilitative exercises in treating mild lumbar disc herniation, strengthening associated muscles, ligaments, and tendons. The researcher hypothesizes that these exercises will positively influence lower back rehabilitation, restore the anatomical alignment of the lumbar vertebrae, improve mobility, and alleviate pain. Pre-tests were conducted before implementing the rehabilitation program, followed by post-tests on the study sample to measure the program’s effectiveness. A series of physical tests, in addition to medical diagnostics, were applied.
After analyzing the post-test results and statistical data, the researcher concluded that the designed rehabilitation program and exercises have a positive effect on the rehabilitation of the lumbar vertebrae and their associated muscles. The researcher recommends adopting this program for the rehabilitation of both athletic and non-athletic wheelchair users suffering from lower back pain.
The study sample consisted of seven individuals with disabilities participating in various sports. Pre-tests, post-tests, and the rehabilitation program were conducted at Al- Razi Center for Physical Therapy from 01/8/2025, to 20/09/2025.
METHODOLOGY
Research Method
The researcher employed the experimental method using a single-group pre-test/post- test design, as it is most suitable for addressing the research problem.
Research Sample
The research sample consisted of a group of athletes with disabilities who are wheelchair users and participate in various sports for individuals with disabilities. All participants suffered from lower back pain and were diagnosed with mild lumbar disc herniation. The sample included seven male athletes aged between 19 and 25 years at the start of the program.

It appears that all skewness coefficient values ranged between 0.83 and 1.76. These values fall within the ±3 range of the curve, indicating the homogeneity of the sample members in these variables and indicators.
Research Tools
1. Electronic spinal decompression device (DRX9000)
2. Infrared imaging device
3. X-ray machine
4. Laser heating device
5. Mats
6. Elastic bands
7. Stopwatch
8. Iron bar with weight plates of different sizes
Research Tests
1. X-ray Examination conducted by the physician.
2. Pain Level Test conducted by the physician.
3. Back Muscle Strength Endurance Test (Ali Salman Abdul-Tarafi, 2013)
• Test: Lifting the body from a prone position on the stomach.
• Objective: To measure the endurance of the back muscles.
• Procedure: From a prone position on the stomach, with arms behind the head and
the thighs stabilized, the participant bends the trunk backward.
• Recording Method: The movement is repeated, and the maximum number of
repetitions is recorded.
4. Flexibility Test (Marwan Abdul-Majid Ibrahim, 2002)
• Test: Trunk backward bending from a prone position.
• Objective: To measure spinal flexibility.
• Tools Used: Measuring ruler.
• Procedure: From a prone position on the stomach, with arms behind the head, the
participant bends the trunk backward to the maximum range.
• Recording Method: The researcher measures the distance from the chin to the ground
using the ruler.
5. Pre-Tests
The pre-test measurements were conducted on 1/8/2025 for the research sample
consisting of 7 wheelchair users suffering from mild lumbar disc herniation and lower back
pain. All data were recorded for subsequent statistical analysis (Kumar, 2023).
6. Post-Tests
The post-test measurements were conducted on the research sample after completing
the rehabilitation program on 19/9/2025. All data were recorded for statistical processing.
7. Rehabilitation Program
The rehabilitation program started on 2/8/2025 and concluded on 20/9/2025.
8. Statistical Tools
The following statistical tools were used:

Result and Discussion
Presentation, analysis, and discussion of the pain level test results

Based on the results presented in the table above and after applying the t-test for differences between the pre-test and post-test, the calculated t-value (8.6) was greater than the tabulated value (2.44). This indicates a significant difference between the pre-test and post-test in favor of the post-test (Hasan, 2020).
The pain level test is one of the medical examinations conducted on the research sample, in addition to X-ray examinations, which were relied upon by the supervising physician to diagnose the injury and determine its severity. The researcher also used these examinations to evaluate the rehabilitation program through pre- and post-tests on the research sample (Zhu, 2024).
The results were positive, showing substantial improvement in the medical assessments. The joint ligaments were in very good condition, and the partial tears present before the program—caused by muscular weakness in the lower back and trunk—were no longer observed in the post-test examinations. This was evident from the improved range of motion, elimination of pain, and restoration of the vertebrae to their anatomical positions, which was clearly visible in the X-rays of the lower back for all participants.
“Muscular strength provides the individual with a cohesive physical structure in all basic movements, whether standing or sitting, and also serves as a preventive and therapeutic measure against bodily deformities and defects” (Abdul-Maleh et al, 2011).
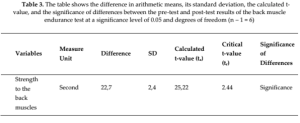
Presentation, Analysis, and Discussion of Back Muscle Endurance Test Results

The results in the table above, after applying the t-test to compare the pre-test and
post-test for the back muscle endurance test, show that the calculated t-value (23.16) is
greater than the tabulated value (2.44). This indicates a highly significant difference between
the pre-test and post-test results, in favor of the post-test (Poliwoda, 2022).
The improvement in back muscle endurance is attributed to the positive effect of the
rehabilitation exercises on the back muscles, especially after using weights. As noted by
Hussein Abu Al-Ruz (1989), “rehabilitation exercises increase the muscular strength of weak
muscles and prevent their atrophy.”
The rehabilitation program included various exercises designed to develop and
enhance endurance. The program began with exercises using light resistance, gradually
increasing the weights and resistance while ensuring that no complications or injuries
occurred during the exercises (Pennington, 2024).
Presentation, Analysis, and Discussion of the Flexibility Test Results
From Table (4), using the t-test for the back flexibility test, the calculated t-value reached 42.72, which is higher than the tabulated t-value of 2.44, indicating significant differences between the pre-test and post-test results in favor of the post-test.
The results in the table show a notable improvement in flexibility, as reflected by the paired-sample t-test. The improvement in the back bending test is attributed to the effectiveness of the rehabilitation program, which included a series of exercises that enhanced the flexibility of the ligaments between the vertebrae. As noted by Qasim Hassan Hussein & Abdul Ali Naseef (1980): “Proper and organized training helps increase the ability of ligaments and tendons to stretch, thus allowing greater range and ease of motion in the joints and developing flexibility.”
The researcher also attributes the observed improvement in the participants’ back strength and flexibility to the integration and progression of exercises from the start of the rehabilitation program, which included a wide range of exercises at varying levels, gradually adapted to the participants’ capacity, helping the body restore its pre-injury state. As confirmed by Marwa Al-Sayed Youssef (1998): “One of the goals of rehabilitation exercises is to return the injured part to its natural state by restoring strength to the muscles acting on the joints and increasing ligament flexibility.”
Additionally, Dalton (2010) noted that most cases of spinal deformities are caused by poor habits in standing, sitting, work posture, or incorrect seating positions, leading to imbalance of forces on both sides of the body, which in turn disrupts the spinal mechanics (Baranidharan, 2024).
CONCLUSIONs
Based on the research results, the researcher reached the following conclusions:
1. The rehabilitation program has a positive effect in rehabilitating mild lumbar disc herniation and relieving lower back pain.
2. There was an improvement in muscular strength and flexibility of the spinal vertebrae among the sample participants as a result of using the prepared rehabilitation program.
RECOMMENDATIONS
The researcher provides several recommendations, including:
1. The importance of using the prepared rehabilitation program in rehabilitating mild lumbar disc herniation and lower back pain.
2. The necessity of preparing specialized training programs for individuals with disabilities that consider their physical condition, ensuring proper body development to achieve good performance and prevent injuries.
3. The importance of keeping up with the use of modern equipment and methods in rehabilitating individuals with disabilities.
REHABILITATION PROGRAM
Week 1: 4 rehabilitation sessions per week / total duration per session: 100 minutes
Sample Session for Week 1
(Exercise repetition: 5×5 / rest between exercises: 2 minutes / rest between sets: 10 seconds)
1. Infrared therapy device – 10 minutes
2. Electronic spinal traction device (DRX9000) – used exclusively by the specialized therapist
3. Backward trunk bending to the maximum range from prone position – 10 minutes
4. Backward trunk bending and returning with alternating arm lifts and lowers from prone position – 15 minutes
5. Hip elevation against the wall / lying on the back – 10 minutes
6. Forward trunk bending from sitting on the bench with stabilization at the hip – 10 minutes
7. Trunk lifting to the level of the bench or higher, with the player in prone position and trunk extending beyond the edge of the bench, assisted by a partner for stabilization
8. Forward and backward trunk bending with the player lying on the back
9. Forward trunk bending and holding the position for 15 seconds
10. Lifting the body from the chair using wooden arm supports on either side of the chair, through arm extension and flexion
Week 2: 4 rehabilitation sessions per week / total duration per session: 100 minutes
Sample Session for Week 2
(Exercise repetition: 10×5 / rest between exercises: 2 minutes / rest between sets: 10 seconds / duration
per exercise: 10 minutes)
1. Infrared therapy device – 10 minutes
2. Electronic spinal traction device (DRX9000) – used exclusively by the specialized therapist
3. Trunk rotation to the right and left alternately while holding a 2 kg weight in each hand, with the patient in a supine position
4. Holding a 2 kg weight in both hands while rotating the trunk to the right and left, with the patient in a supine position and arms raised overhead
5. Pulley device chest-level pull from a seated position, with a 5 kg weight
6. Lifting a 7 kg weight with both hands from the floor, with the patient seated on a bench
7. Lifting a 7 kg weight with both hands to head level from prone position on the bench, arms extended forward
8. Backward trunk bending with a 5 kg weight on the back, patient in prone position
9. Raising and lowering a 3 kg weight with full arm extension and maximum backward return, patient lying on the side
10. Repeat the previous exercise for the opposite side
Week 3: 4 rehabilitation sessions per week / total duration per session: 100 minutes
Sample Session for Week 3
(Exercise repetition: 10×5 / rest between exercises: 2 minutes / rest between sets: 10 seconds / duration
per exercise: 10 minutes)
1. Infrared therapy device – 10 minutes
2. Electronic spinal traction device (DRX9000) – used exclusively by the specialized therapist
3. Trunk rotation to the right and left while holding a 5 kg weight in each hand, patient in supine position
4. Pulley device chest-level pull with both hands, using a 12 kg weight
5. Backward trunk bending with a 7 kg weight placed on the back, patient in prone position
6. Raising and lowering a 3 kg weight with the arm, patient lying on the side
7. Repeat the previous exercise for the opposite side
8. Wheelchair sprinting between cones for a distance of 15 meters, back and forth
9. Lifting a 15 kg weight with both hands to head level, patient in supine position on the bench
10. Back massage – 10 minute
Week 4: 4 rehabilitation sessions per week / total duration per session: 100 minutes
Sample Session for Week 4
(Exercise repetition: 5×5 / rest between exercises: 2 minutes / rest between sets: 10 seconds / duration per exercise: 10 minutes)
1. Infrared therapy device – 10 minutes
2. Electronic spinal traction device (DRX9000) – used exclusively by the specialized therapist
3. Lifting a 12 kg weight with both hands to head level, patient in prone position on the bench, arms extended forward
4. Backward trunk bending with an 8 kg weight placed on the back, patient in prone position
5. Raising and lowering a 3 kg weight with the arm, patient lying on the side, head supported by one hand
6. Repeat the previous exercise for the opposite side
7. Pulley device lower-level pull with both hands, patient in 45° prone position, using a 10 kg weight
8. Pull-ups using a bar from the wheelchair
9. Wheelchair sprinting between cones for a distance of 15 meters, back and forth
10. Back massage – 10 minutes
Week 5: 4 rehabilitation sessions per week / total duration per session: 100 minutes
Sample Session for Week 5
(Exercise repetition: 5×5 / rest between exercises: 2 minutes / rest between sets: 10 seconds / duration per exercise: 10 minutes)
1. Infrared therapy device – 10 minutes
2. Electronic spinal traction device (DRX9000) – used exclusively by the specialized therapist
3. Lifting a 12 kg weight with both arms from the floor to the abdomen, patient seated in the wheelchair
4. Lifting a 10 kg weight with both hands to head level, patient in prone position on the bench
5. Placing a 7 kg weight on the back and bending the trunk backward, patient in prone position
6. Raising and lowering a 4 kg weight with the arm, patient lying on the side, fully extending and returning the arm backward to the maximum range
7. Repeat the previous exercise for the opposite side
8. Pulling with both hands on the pulley device from an inclined prone position with a 15 kg weight
9. Hanging from a pull-up bar, patient seated in the wheelchair
10. General body massage with emphasis on back muscles
Weeks 6 & 7: 4 rehabilitation sessions per week / total duration per session: 100 minutes
Sample Session for Weeks 6 & 7
(Exercise repetition: 5×5 / rest between exercises: 2 minutes / rest between sets: 10 seconds / duration per exercise: 10 minutes)
1. Infrared therapy device – 10 minutes
2. Electronic spinal traction device (DRX9000) – used exclusively by the specialized therapist
3. Pulling with both hands on the pulley device with a 25 kg weight, patient seated
4. Lifting a 25 kg weight from the floor to chest level, patient seated in the wheelchair
5. Zigzag wheelchair running between cones over a distance of 20 meters
6. Lifting a 25 kg weight with both hands to head level, patient in prone position on the bench, arms extended forward
7. Raising and lowering a 4 kg weight with one arm, patient lying on the side, fully extending the arm and returning it backward to the maximum range
8. Repeat the previous exercise for the opposite side
9. Pulling with both hands on the pulley device from a 45-degree inclined position with a 25 kg weight
10. Massage of the lower back region
References
Abdul Malah, F., et al. (2011). Sports training for second-stage students. Amman: Arab Society Library for Publishing and Distribution.
Abdul-Majid Ibrahim, M. (2002). Volleyball for physically disabled – sitting. Amman: Al- Warraq Publishing and Distribution.
Abdul-Tarfi, A. S. (2013). Applied tests in physical education: Motor, physical, and skill assessments. Baghdad: Dar Al-Kutub wa Al-Watha’iq.
Abu Al-Raz, H. (1989). Effect of a proposed physical exercise program on some motor abilities and postural deviations of physically disabled individuals (Unpublished PhD thesis). Helwan University, Faculty of Physical Education.
Al-Kinani, A. K. (2009). Introduction to statistics and applications with SPSS. Baghdad: Dar Al-Dhia Printing House.
Al-Sayed Youssef, M. (1998). Studies on problems of sports medicine. Alexandria: Al-Ishaa Technical Library and Press.
Al-Talib, N., & Al-Samarrai, M. (1987). Principles of statistics and physical and sports tests. University of Mosul: Dar Al-Kutub for Printing and Publishing.
Baranidharan, G. (2024). 24-month outcomes of indirect decompression using a minimally invasive interspinous fixation device versus standard open direct decompression for lumbar spinal stenosis: A prospective comparison. Journal of Pain Research, 17, 2079–2097. https://doi.org/10.2147/JPR.S453343
Dalton, E. (2005). Advanced myoskeletal techniques. Oklahoma City, OK: Freedom From Pain Institutes.
Guzmán, A. M. Diago. (2025). Not surgical manage of discal hernia with the DRX9000 in Portoviejo, Ecuador. Revista Habanera de Ciencias Médicas, 24.
https://www.scopus.com/inward/record.uri?partnerID=HzOxMe3b&scp=1050148083
21&origin=inward
Hasan, S. (2020). Interspinous and interlaminar devices for decompression. In Minimally invasive spine surgery: Surgical techniques and disease management (pp. 189–199).
https://doi.org/10.1007/978-3-030-19007-1_18
Hassan Hussein, Q., & Naseef, A. A. (1980). Science of sports training. Mosul: Dar Al-Kutub for Printing and Publishing.
Kumar, N. (2023). Evaluating 5-year outcomes of interlaminar devices as an adjunct to decompression for symptomatic lumbar spinal stenosis. European Spine Journal, 32(4), 1367–1374. https://doi.org/10.1007/s00586-023-07610-x
Li, H. (2025). Treatment of spinal cervical spondylosis with ‘Uni-C’ device and anterior cervical discectomy and decompression fusion. Journal of the College of Physicians and Surgeons Pakistan, 35(5), 675–676. https://doi.org/10.29271/jcpsp.2025.05.675
Pennington, Z. (2024). Decompression alone versus interspinous/interlaminar device placement for degenerative lumbar pathologies: Systematic review and meta-analysis. World Neurosurgery, 185, 417–434. https://doi.org/10.1016/j.wneu.2024.03.054
Poliwoda, S. (2022). A minimally invasive lumbar decompression procedure after an interspinous spacer device implantation: An uncommon order of treatment with a successful outcome. Orthopedic Reviews, 14(4). https://doi.org/10.52965/001c.35844
Schenck, C. D. (2022). Interspinous process device versus conventional decompression for lumbar spinal stenosis: 5-year results of a randomized controlled trial. Journal of Neurosurgery: Spine, 36(6), 909–917. https://doi.org/10.3171/2021.8.SPINE21419
Yassin, W., & Abdul-Abidi, H. M. (1996). Statistical applications in physical education research. Mosul: Dar Al-Kutub for Printing and Publishing.
Zhang, Y. (2021). Which is the most effective treatment for lumbar spinal stenosis: Decompression, fusion, or interspinous process device? A Bayesian network meta- analysis. Journal of Orthopaedic Translation, 26, 45–53. https://doi.org/10.1016/j.jot.2020.07.003
Zhu, C. (2024). Efficacy and safety of interspinous process device compared with alone decompression for lumbar spinal stenosis: A systematic review and meta-analysis. Medicine United States, 103(23). https://doi.org/10.1097/MD.0000000000038370